PATHOLOGIES OF THE LUNGS
Smoking-Associated Lung Cancer
Lung cancer stands as the most common cause of cancer-related deaths globally, claiming a staggering 1.76 million lives each year. Tobacco use, as numerous studies have shown, plays a pivotal role in this grim reality. According to research published in The Lancet, approximately 22% of cancer deaths are attributable to tobacco use.
The correlation between smoking and lung cancer is undeniable.
In fact, an estimated 90% of lung cancer cases can be directly
linked to tobacco consumption. And it's not just the nicotine in
cigarettes that's the culprit here. The secondary components of
cigarette smoke, including carbon monoxide and tar, play
significant roles in causing harm to the lungs. Carbon monoxide,
for instance, interferes with the blood's ability to carry oxygen,
while tar, a complex mixture of chemicals apart from nicotine
and carbon monoxide, is laden with carcinogens.
Carcinogens such as polycyclic aromatic hydrocarbons,
N-nitrosamines, and aromatic amines, among others, wreak
havoc on lung tissue, leading to the development of cancerous
cells. And what's more concerning is that these carcinogens
can be detected not only in the lungs but also in bodily fluids
like urine, blood, and breath, underscoring the pervasive
damage caused by smoking.
The repercussions of lung cancer extend beyond the lungs themselves. Metastasis, the spread of cancer to distant sites, can occur in various organs, including the brain, bones, liver, and adrenal glands. Despite advances in treatment, advanced-stage lung cancer often poses significant challenges in terms of management and prognosis.
By understanding the intricate mechanisms linking smoking to lung cancer and spreading awareness about the risks involved, we can strive towards reducing the burden of this devastating disease.It's imperative that we continue to educate individuals about the detrimental effects of tobacco use and advocate for policies aimed at curbing its prevalence. Through ongoing research and public health initiatives, we can work towards a future where lung cancer ceases to be a leading cause of mortality worldwide.

Lung affected by lung cancer. Photo Credit: Human Protein Atlas
Small cell carcinoma is a high-grade neuroendocrine tumor that predominantly arises in the hilum of smokers. It's characterized by its aggressive nature and poor prognosis, with limited targeted therapy options currently available.
Small cell carcinoma is associated almost exclusively with smoking or tobacco exposure, constituting around 10-15% of all lung cancer cases. A striking 70% of patients present with metastasis at the time of diagnosis, underscoring the advanced stage at which this cancer is often detected. Common sites of metastasis include the liver, adrenals, bone, bone marrow, and brain. Additionally, small cell carcinoma typically arises from the neuroendocrine cells of the basal bronchial epithelium.
Diagnosis relies heavily on biopsy findings, with characteristic hematoxylin and eosin morphology guiding the process. Staging is typically conducted via radiological imaging, such as chest CT scans, brain MRIs, or bone scans.
Symptoms can vary but often include:
-
Cough
-
Dyspnea
-
Weight loss
-
Paraneoplastic syndromes such as Cushing syndrome and superior vena cava syndrome.
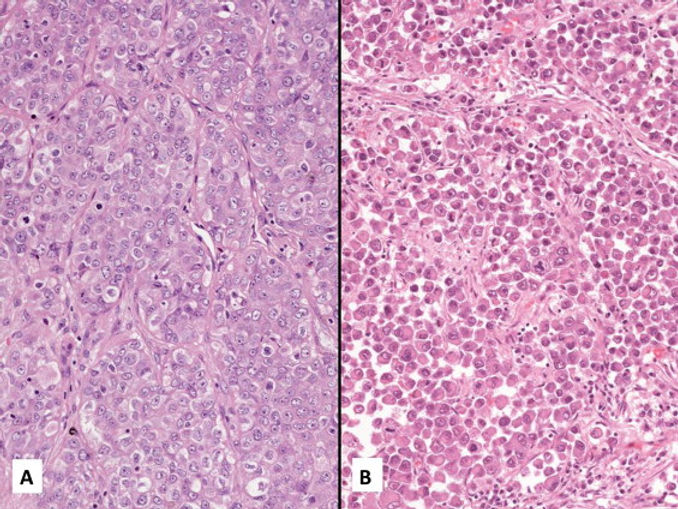
From a pathological standpoint, small cell carcinoma presents as a mass of white-tan soft friable necrosis, with peripheral nodules displaying a circumscribed, fleshy cut surface. Microscopically, it's characterized by round or oval blue cells with minimal cytoplasm, along with distinctive nuclear features and patterns such as sheets, clusters, and rosettes. Prognosis tends to be more favorable in women, although overall survival rates remain relatively low. Treatment typically involves combined chemotherapy, often platinum-based, and radiation therapy. Unfortunately, targeted immunotherapy options are currently lacking.

Female, 78, small cell lung carcinoma. Photo Credit: The Human Protein Atlas


Test Your Knowledge
1. What are the main histologic patterns associated with adenocarcinoma?
a) Squamous, sarcomatoid, and neuroendocrine
b) Acinar, papillary, micropapillary, lepidic, and solid
c) Small cell, large cell, and bronchioloalveolar
d) Clear cell, chromophobe, and oncocytic
2. What is a significant risk factor for adenocarcinoma besides smoking?
a) Exposure to radon gas
b) Consumption of grilled meat
c) Exposure to secondhand smoke, cooking oil fumes, and asbestos
d) Lack of physical exercise
3. Which of the following is NOT typically a clinical presentation of adenocarcinoma?
a) Cough
b) Hemoptysis
c) Dyspnea
d) Palpitations
4. Which of the following is NOT a characteristic feature of large cell carcinoma on histological examination?
a) Sheets or solid nests of round to polygonal cells
b) Prominent nucleoli
c) Thin fibrous capsules
d) Moderately abundant cytoplasm
5. What is the primary method for diagnosing large cell carcinoma?
a) Blood tests
b) Genetic testing
c) Radiological imaging, histological examination, and immunohistochemical analysis
d) Urine analysis
6. What percentage of non-small cell lung carcinomas does squamous cell carcinoma account for?
a) Approximately 10%
b) Roughly 30%
c) Roughly 10%
d) Approximately 40%
7. Which diagnostic method is typically used to evaluate lung cancer?
a) CT scans
b) X-rays
c) Blood Test
d) MRI scans
8. What are common characteristics observed in squamous cell carcinoma on microscopy?
a) Glandular formation
b) Keratinization, intercellular bridging, inflammation, and necrosis
c) Papillary structures
d) Mucin production